Cholesterol, cardio and statins...

A related question that often comes up in metabolic clinics is whether a particular cholesterol result is genuinely worrisome. The short answer: it depends on context.
What Cholesterol Actually Is
Cholesterol is a waxy, fat‑like molecule used in cell membranes and as the building block for all steroid hormones, including testosterone, oestrogen, cortisol and aldosterone.
In steroid‑producing tissues (for example Leydig cells in the testes), cholesterol is converted to pregnenolone and then to testosterone under luteinising‑hormone (LH) control.
So cholesterol is not “all bad” – the issue is how much is carried in atherogenic particles and how long those particles spend in your arteries.
Why Cholesterol Got a Bad Reputation
From the 1980s onwards, large population studies and trials linked higher LDL‑cholesterol and apoB‑containing lipoproteins to coronary heart disease, driving low‑fat dietary advice and aggressive cholesterol‑lowering strategies.
We now know it is the burden of apoB‑containing particles (LDL, VLDL remnants, IDL, Lp(a)) that is causally linked to atherosclerotic cardiovascular disease, not dietary cholesterol alone.
LDL, HDL, VLDL, apoB and Triglycerides – What’s the Difference?
Think of “cholesterol” as cargo carried in different lipoprotein particles:
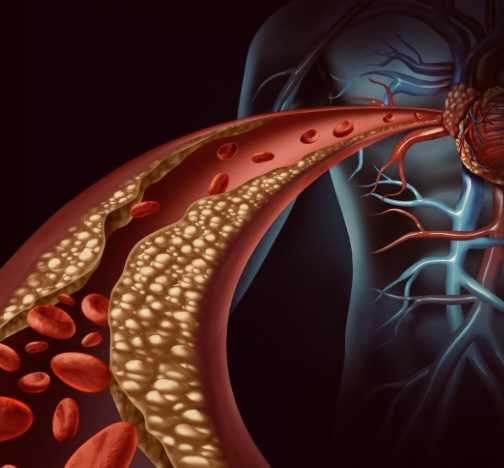
- LDL (“bad cholesterol”) – Cholesterol‑rich particles containing apoB that deliver cholesterol to tissues and can penetrate the arterial wall; long‑term elevated LDL is strongly causal for atherosclerotic disease.
- VLDL – Triglyceride‑rich apoB particles made by the liver; as they are metabolised to remnants and LDL, their cholesterol content explains a large part of the myocardial‑infarction risk linked to apoB particles.
- HDL (“good cholesterol”) – Involved in reverse cholesterol transport; higher HDL‑C is associated with lower risk observationally, but trials of HDL‑raising drugs have not consistently reduced events, so HDL is more a marker of metabolic health than a simple “good” number.
- Apolipoprotein B (apoB) – There is one apoB per atherogenic particle; apoB therefore reflects the total number of LDL, VLDL, IDL and Lp(a) particles and often tracks risk better than LDL‑C alone.
- Triglycerides – Carried mainly in VLDL and chylomicrons; elevated levels mark excess triglyceride‑rich remnants and insulin resistance and are independently associated with higher CV risk.
ApoB‑containing particles (LDL, VLDL remnants) are directly causal for plaque, whereas HDL is more of a health proxy.
Statins and “Number Needed to Treat”
Statins reduce liver cholesterol synthesis, up‑regulate LDL receptors, and lower LDL‑C and apoB particles, leading to fewer cardiovascular events.
The number needed to treat (NNT) over about 5–10 years depends heavily on your baseline risk:
- In low‑risk primary‑prevention patients, 5‑year NNTs can be >100.
- In higher‑risk groups, NNTs fall to around 30–40 or lower, meaning much greater absolute benefit.
The same LDL level in two people can therefore mean very different treatment value depending on overall risk.
QRISK, HbA1c and Blood Pressure – Looking at the Whole Picture
In the UK, QRISK3 is the standard 10‑year cardiovascular‑risk calculator used in primary care. It incorporates:
- Age, sex, ethnicity, deprivation
- Smoking, blood pressure, total and HDL cholesterol
- Diabetes status, chronic kidney disease, rheumatoid arthritis, atrial fibrillation, and certain medications
Patients can estimate their risk via the public QRISK3 tool, but interpretation should be done with a clinician.
- HbA1c/glucose – Higher HbA1c (pre‑diabetes or diabetes) reflects chronic hyperglycaemia and is a strong cardiovascular‑risk factor.
- Blood pressure – Elevated BP damages arteries and increases risk of stroke and heart attack; it is a core QRISK input and major treatment target.
Two people with identical cholesterol can sit on different sides of the statin‑treatment threshold depending on HbA1c, BP, smoking and other factors.
Lifestyle, Supplements and Cholesterol
Exercise
Regular aerobic exercise:
- Modestly increases HDL‑C
- Reduces LDL‑C and total cholesterol
- Improves triglyceride clearance, especially in dyslipidaemia
- Also improves insulin sensitivity, blood pressure and body composition, all of which reduce overall CV risk.
Berberine
- Meta‑analytic data suggest berberine can lower LDL‑C, total cholesterol and triglycerides and modestly improve weight indices.
- It should be seen as an adjunct, not a replacement for statins in high‑risk patients, and used with medical oversight because of possible interactions and variable supplement quality.
Fish Oils (Omega‑3)
- Omega‑3 fatty acids primarily lower triglycerides by reducing hepatic VLDL production and increasing clearance.
- They show modest reductions in coronary events in some analyses, but effects on LDL‑C and HDL‑C are small and inconsistent.
Dietary patterns (e.g. Mediterranean‑style diet, reduced refined carbohydrates and trans fats, adequate fibre) also help lower atherogenic lipoproteins and improve glycaemia, but are not substitutes for statins where these are clearly indicated.
So… Is Your Cholesterol a Problem?
The honest answer is: it depends.
It depends on:
- Your apoB/LDL‑C, triglyceride and Lp(a) levels
- Your QRISK‑estimated 10‑year risk, shaped by age, sex, family history, HbA1c/diabetes, blood pressure, smoking and co‑morbidities
- Your genetics, body composition and lifestyle (exercise, diet, alcohol, sleep)
For one person, a modest LDL elevation with low QRISK, excellent BP and HbA1c and an active lifestyle may justify a focus on lifestyle plus monitoring.
For another with the same LDL but high QRISK, hypertension and pre‑diabetes, statins plus lifestyle may offer substantial absolute benefit.
- Lilly’s phase 2 retatrutide results – NEJM
https://investor.lilly.com/news-releases/news-release-details/lillys-phase-2-retatrutide-results-published-new-england-journal - Retatrutide UK availability and legal status – Lola Health
https://lolahealth.com/blogs/longevity/retatrutide-uk-availability - Comparison of semaglutide, tirzepatide and retatrutide (mechanisms, efficacy) – Nature
https://www.nature.com/articles/s41366-026-02025-2 - Phase 2 GIP/GLP‑1/glucagon agonist trial summary – Pace-CME
https://pace-cme.org/news/results-of-phase-2-trial-with-gip-glp-1-and-glucagon-receptor-agonist-to-treat-obesity/2456473/ - Phase 2 retatrutide in obesity, type 2 diabetes and NASH – ADA Meeting News
https://www.adameetingnews.org/phase-2-trial-results-demonstrate-benefits-of-retatrutide-in-obesity-type-2-diabetes-nash/ - Triple G agonists editorial – New England Journal of Medicine
https://www.ovid.com/journals/nejm/abstract/10.1056/nejme2307282~triple-g-agonists-a-home-run-for-obesity - Retatrutide – “Game changer” obesity pharmacotherapy review (PMC)
https://pmc.ncbi.nlm.nih.gov/articles/PMC12190491/ - Retatrutide – “Game changer” obesity pharmacotherapy review (PubMed)
https://pubmed.ncbi.nlm.nih.gov/40563436/ - Triple‑hormone‑receptor agonist retatrutide for obesity – NEJM correspondence
https://www.ovid.com/journals/nejm/abstract/10.1056/nejmc2310645~triple-hormone-receptor-agonist-retatrutide-for-obesity - Retatrutide clinical trials and TRIUMPH programme – Lola Health
https://lolahealth.com/blogs/longevity/retatrutide-clinical-trials - Retatrutide UK legal status – Vitality Peptides
https://vitalitypeptides.co.uk/retatrutide-uk-legal-status-2025/ - Retatrutide vs semaglutide comparison – Lola Health
https://lolahealth.com/blogs/longevity/retatrutide-vs-semaglutide-comparison - Semaglutide vs tirzepatide vs retatrutide overview – NDA Medical Spa
https://ndamedicalspa.com/blogs/medical-spa/semaglutide-vs-tirzepatide-vs-retatrutide-which-weight-loss-treatment-is-right-for-you - Triple‑hormone‑receptor agonist retatrutide for obesity – PDF review
https://sio-obesita.org/wp-content/uploads/2023/12/del-prete-2.pdf - Retatrutide vs tirzepatide vs semaglutide comparison – Voy
https://www.joinvoy.com/blog/retatrutide-vs-tirzepatide-vs-semaglutide - QRISK3 main site
https://qrisk.org - QRISK3 calculator (Patient.info)
https://patient.info/doctor/cardiovascular-disease/qrisk3-cardiovascular-risk-calculator - Cellular cholesterol delivery and utilisation – PMC
https://pmc.ncbi.nlm.nih.gov/articles/PMC2890697/ - Metabolic profiling of cholesterol and sex steroid hormones – PMC
https://pmc.ncbi.nlm.nih.gov/articles/PMC5064754/ - Hormonal regulation of testicular steroid and cholesterol – PMC
https://pmc.ncbi.nlm.nih.gov/articles/PMC2262169/ - Hormonal regulation of testicular steroid and cholesterol – PubMed
https://pubmed.ncbi.nlm.nih.gov/18032697/ - Lipid molecules – steroids (general biology text)
https://bio.libretexts.org/Bookshelves/Introductory_and_General_Biology/General_Biology_(Boundless)/03:Biological_Macromolecules/3.06:_Lipid_Molecules-_Steroids - Triglycerides and cardiovascular risk – apoB commentary (EAS)
https://eas-society.org/page/commentary-triglycerides-and-cardiovascular-risk-apolipoprotein-b-holds-the-key/ - VLDL cholesterol and MI risk – Pace-CME
https://pace-cme.org/news/vldl-cholesterol-explains-half-of-mi-risk-from-apob-containing-lipoproteins/2455872/ - Impact of aerobic exercise on HDL – PMC
https://pmc.ncbi.nlm.nih.gov/articles/PMC10003711/ - Statin use in primary prevention – JAMA Cardiology
https://jamanetwork.com/journals/jamacardiology/fullarticle/2752379 - Number needed to treat for statins in primary care – Family Practice
https://academic.oup.com/fampra/article/35/4/376/4756505 - Berberine supplementation and lipid profile – umbrella review
https://www.sciencedirect.com/science/article/abs/pii/S2213434423000361 - Fish oil and cardiovascular risk – GP Notebook
https://gpnotebook.com/pages/cardiovascular-medicine/efficacy-of-using-fish-oil-to-reduce-cardiovascular-risk - Cholesterol and testosterone overview (patient‑friendly explainer)
https://www.hims.com/blog/cholesterol-and-testosterone
Join Our Wellness Community
Subscribe for the latest insights on aesthetics, health tips, and exclusive offers from Eden Clinic.
